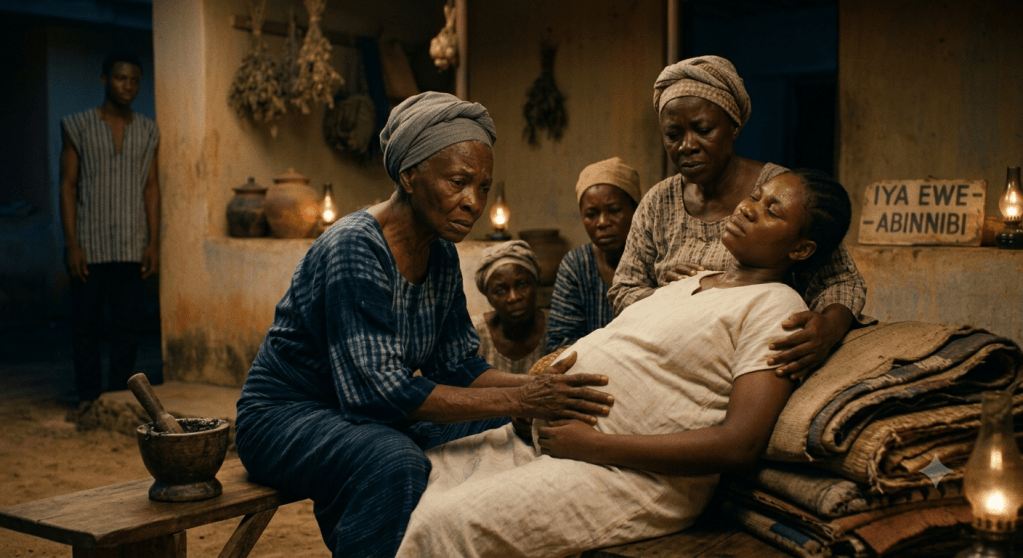
The labour had gone on for hours.
The baby’s head had not appeared.
The woman’s cries had become weaker.
Around her, family members waited anxiously, wondering why nothing seemed to be happening.
If this story had unfolded inside a modern hospital, the conversation might have turned immediately to cervical dilation, fetal position, or the possibility of a Caesarean section.
But that was not the first question the traditional birth attendant asked.
When I interviewed one experienced Yoruba midwife during my fieldwork, she told me something I have not forgotten.
“When a woman’s labour is delayed,” she said, “I first ask why.”
She explained that not every prolonged labour has the same cause. Some, she believed, arise from physical complications. Others require understanding something beyond what the eyes can see.
Only after deciding what kind of problem she was dealing with would she begin treatment.
She described her process quietly, almost as though it were the most ordinary thing in the world.
If she concluded that the obstruction was spiritual, she would first turn her own clothes inside out before putting them back on.
Then she would change the mother’s position.
Only then would she prepare the herbs.
Around her home grew plants she had cultivated over many years, not simply because they were medicinal, but because she trusted them.
She would pluck fresh leaves of Ewe Lapalapa, Ewe Ewuro, and Ajekobale, pound them together with traditional black soap, and prepare a herbal bath.
To an outsider, it might seem like a collection of unrelated actions.
To her, every step belonged to the same system of care.
What fascinated me most was not whether someone reading this believes in spiritual causes of prolonged labour.
It was the clinical logic behind her practice.
She did not begin with treatment.
She began with diagnosis.
She believed that effective care depended on correctly understanding the nature of the problem before choosing the remedy.
That is a principle every healthcare system values, even if different systems define illness in different ways.
Too often, Indigenous healthcare is portrayed as though practitioners simply administer herbs whenever someone falls ill.
My conversations suggested something far more sophisticated.
The herbs were never the starting point.
Observation came first.
Interpretation came next.
Treatment followed.
Whether that treatment involved medicinal plants, changes in posture, ritual actions, or a combination of all three depended on the diagnosis the practitioner reached.
As I left her home that afternoon, I realized that I had spent years thinking of Indigenous medicine as a collection of remedies.
She had quietly shown me something different.

Leave a comment